

1 Introduction
Communication models that prioritise one-way transfer of knowledge over dialogue and inclusion have long been critiqued [CPAS Inclusive Science Communication Collective, 2025], but persist in practice [Seethaler et al., 2019; Simis et al., 2016]. In the context of mental illnesses, transitioning to more participatory approaches is especially important. These disorders are shaped not only by clinical dimensions but also by social factors, arguably understood best by person(s) with lived experience (PwLE). This article contributes to underexplored areas of science communication by examining how participatory, arts-based approaches can centre the expertise of PwLE in communication about mental illnesses.
1.1 Understanding stigma and its consequences
Stigma is a pervasive negative attitude that marks someone with a mental illness as undesirable, incompetent or dangerous. This attitude is built on a false dichotomy of normality, where a diagnosis of mental illness is considered “abnormal” [Corrigan et al., 2014; Gururaj et al., 2016; Shidhaye & Kermode, 2013]. Access to services, education, employment, healthcare and participation in community life becomes limited for PwLE/families [Corrigan & Watson, 2002; Thornicroft et al., 2022], leading to the world’s largest treatment gap in India, where 70–85% of people with a mental illness do not receive adequate care [Gururaj et al., 2016]. Stigma plays a central role in sustaining this gap, creating a loop in which a lack of care both seeds and feeds negative social attitudes.
1.2 Reducing stigma through communication: from deficit to participation
Traditionally, efforts to reduce stigma towards mental illness have focused on the deficit model of communication [Bucchi, 2008; Corrigan, 2020], based on the premise that stigmatising attitudes arise due to a lack of knowledge. Interventions in India, such as mental health literacy modules [Raghavan et al., 2024], community awareness programs and training for healthcare workers, have therefore prioritised education and awareness [Gundi et al., 2025; Kaur et al., 2021; Kirpekar et al., 2024]. While these efforts support treatment-seeking and sensitisation, evidence suggests that they do not necessarily lead to reductions in stigmatising or discriminatory behaviours [Kågström et al., 2025; Majeed et al., 2024; Thornicroft et al., 2016]. Social environments, cultural meanings, and representations in public discourse, including popular media, significantly shape the lived experience of individuals with severe mental illnesses [Edward, 2025]. These limitations highlight the need for approaches that go beyond education and support the understanding of the lived experience of a mental illness.
The participatory model of science communication provides an alternative to the deficit model, emphasising dialogue, mutual learning and multiple forms of knowledge [Metcalfe et al., 2022]. These approaches focus on how communication is structured: who is invited to participate, whose knowledge is considered legitimate and under what conditions dialogue becomes possible [Bucchi & Trench, 2021; Einsiedel, 2021]. Such questions are especially salient when communicating about mental illnesses as prevalent social conditions and perceived risks of engagement tend to sideline the voices of PwLE. These approaches may create spaces that foreground experiential knowledge, thereby enabling engagement where knowledge is shaped through interaction rather than instruction.
The participatory model aligns closely with contact-based approaches to stigma reduction, sharing similar principles of interaction. Grounded in Allport’s intergroup contact hypothesis, this theory posits that under conditions of equal status, cooperation and institutional support, structured interpersonal contact between groups can reduce prejudice [Allport, 1954]. Crucially, a larger meta-analysis of over 500 studies of intergroup contact demonstrated that stigmatising attitudes are diminished even when Allport’s conditions are only partially fulfilled [Pettigrew & Tropp, 2006]. This finding is particularly relevant for low- and middle-income countries (LMICs), where ideal conditions for participation are rarely available, but still, meaningful social contact with PwLE remains possible [Damsté et al., 2024; Mendon et al., 2024; Rai et al., 2023].
Despite the conceptual alignment, evidence of contact theory as a practical framework has been lacking within science communication research. Without such evidence, dialogue- and participation-based communication remains disconnected from a robust body of research. Empirical evidence demonstrates that sustained intergroup contact can reduce bias and improve relations; however, this remains heavily skewed towards high-income countries (HICs) [Thornicroft et al., 2022]. Social conditions and cultural contexts in many LMICs, including India, prevent active participation by PwLE. Here, stigma operates not only via misinformation but also through shame and moral judgement. This shapes anticipated social consequences and influences whether someone with lived experience will choose to speak out. As a result, contact-based formats common in HICs, such as public testimony or peer-led workshops, are not always feasible without intensive adaptation [Kaur et al., 2021; Mendon et al., 2024; Samudre et al., 2016; Shidhaye & Kermode, 2013].
Concurrently, without the involvement of PwLE, efforts to combat stigma using participatory approaches remain incomplete in perspective and inclusivity [Gronholm et al., 2024; Sartor, 2023]. PwLE are frequently positioned only as subjects of care in biomedical narratives and professional hierarchies, with fewer opportunities to be recognised as credible knowledge holders. Embedding lived experience within participatory formats in science communication offers a way to challenge this imbalance. This aligns with calls for more inclusive science communication approaches that focus on people, purpose and content [CPAS Inclusive Science Communication Collective, 2025].
In this Practice Insight, we present a novel approach, integrating participatory models of science communication with contact theory across a series of events using arts-based methods. Reflecting on multiple forms of participant feedback, we explore how dialogue can be made possible while navigating challenges of stigma and uneven participation in the context of mental illnesses. These insights highlight key transitions in mental illness communication: from expert-led deficit-style dissemination to collaborative exchange, from textbook definitions to creative expression, and from tokenism to co-production.
2 Designing creative participatory methods
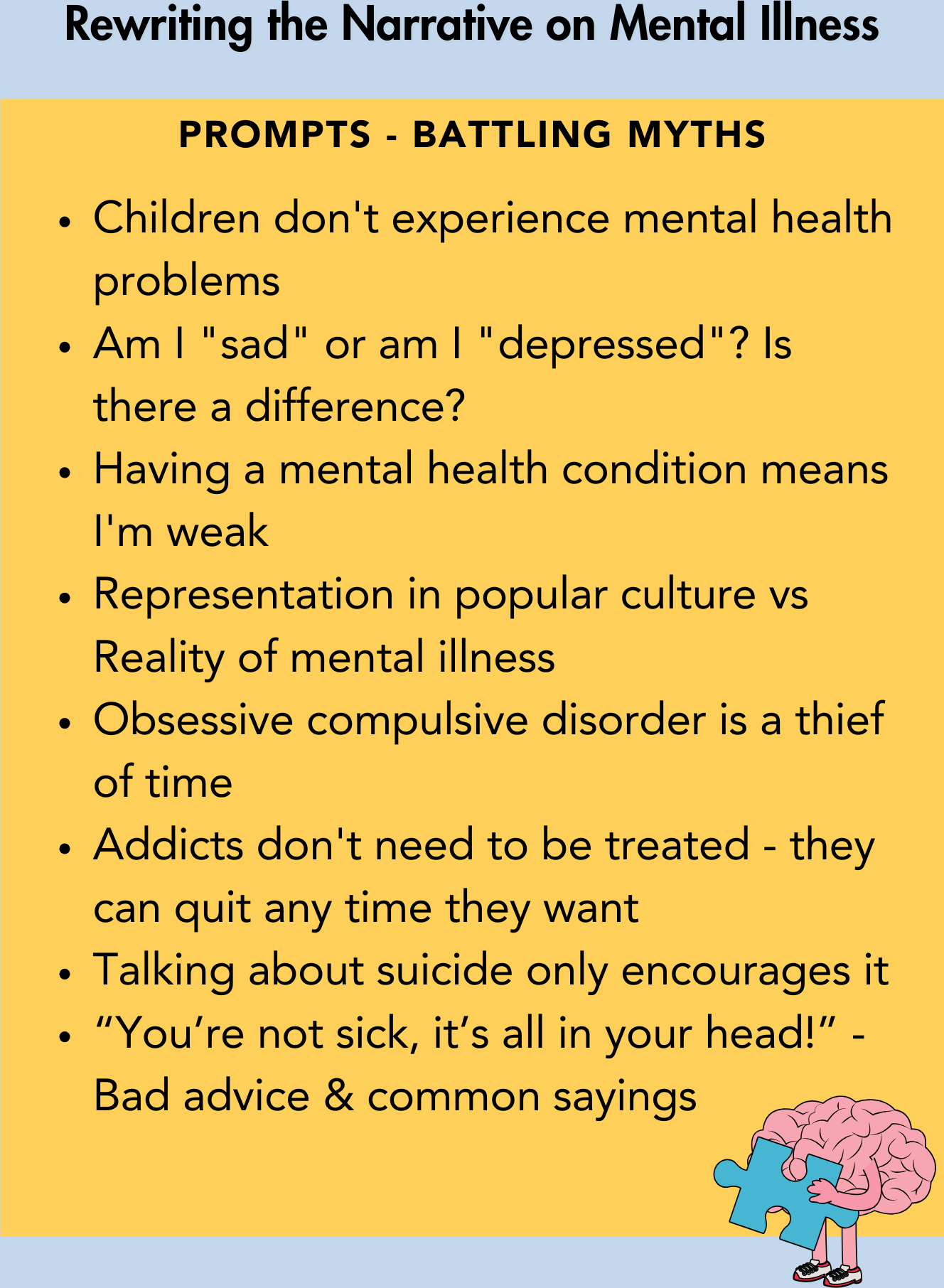
We designed a series of art-based engagements with PwLE, prioritising equal-status, small group interactions. PwLE partners were identified through clinicians, researchers and community networks at the National Institute of Mental Health and Neurosciences, Bengaluru (NIMHANS), the Rohini Nilekani Centre for Brain and Mind — NIMHANS (CBM-NIMHANS), and the Mental Health Support Foundation (MHSF). We held preparatory discussions where PwLE co-created the design of event materials (Figure 1a–b) and conversation prompts (Figure 1c) (Table 1). Across events, we prioritised participant privacy and well-being by offering options for anonymity and access to trained clinician support. Registration and feedback were managed using standard online forms, publicised via our communication channels and at venues.
2.1 “Rewriting the narrative on mental illness” creative expression workshop
We conducted a hybrid workshop at one of India’s largest annual science festivals to discuss how common myths around mental illnesses contribute to stigma. Each session began with inputs from speakers (two psychiatrists [one also a PwLE of ADHD], a scientist, and a PwLE of bipolar disorder), followed by Q&A. Participants responded to prompts (Figure 1c) using their preferred creative medium (e.g., comics, poems, illustrations, skits, etc.) and shared their work with the group at the end.

2.2 Zine-making workshop for World Bipolar Day
This in-person event focused on bipolar disorder and was designed to feature small group discussions centred on dialogue with PwLE.
|
Prompts
directed
towards
PwLE
|
What are some stigmas or misconceptions you faced? How did you overcome them? |
|
How can people be more empathetic to those living with any mental illness? |
|
|
What does your day-to-day feel like? Has it changed since the diagnosis? How does it differ in the various stages of the disorder? |
|
|
What was the disease onset like for you? |
|
|
Were there challenges in the process of getting this diagnosis? Has your life been different in any way, including people’s demeanour towards you, since the diagnosis? |
|
|
What do you wish people understood about living with the disease? |
|
|
What kind of research would be beneficial? |
|
|
Prompts
directed
towards
participants
|
What do you think a person with bipolar disorder looks like? |
|
How do you perceive their behaviour? |
|
|
How do you think you would approach a person with the disorder? |
|
|
Do you think you could identify signs of bipolar disorder, regardless of the length of the interaction? |
|
|
What kind of support do you think a person with bipolar disorder needs? |
|
The workshop began with brief overviews of ongoing research and common misconceptions about bipolar disorder. Next, the workshop facilitator introduced zines as a tool to reflect on personal biases. Participants created zines in response to prompt-based questions (Table 1) using drawings, words and/or phrases. This was followed by small-group conversations, with around 10 participants and a PwLE at each table (Supplementary Figure 1 in the supplementary material). Subsequently, participants revisited the same prompts and depicted whether their understandings had changed.
2.3 Public art exhibitions
We issued an open art call for artistic perspectives on bipolar disorder. Submission required two elements: (i) a digital image of the artwork and (ii) a short description by the artist. Artworks were categorised into the following themes based on the descriptions: Recovery, Struggle, Expression, Identity and Other (if descriptions were insufficient). We obtained consent for display, giving artists the option to remain anonymous.
Our first art exhibition, held on World Bipolar Day, accompanied the zine-making workshop and included received submissions alongside pieces created by people with disabilities at a workshop conducted by NIMHANS in association with the Department of Empowerment of Persons with Disabilities, Government of India. We also invited local, featured artists to visit and interact with participants.
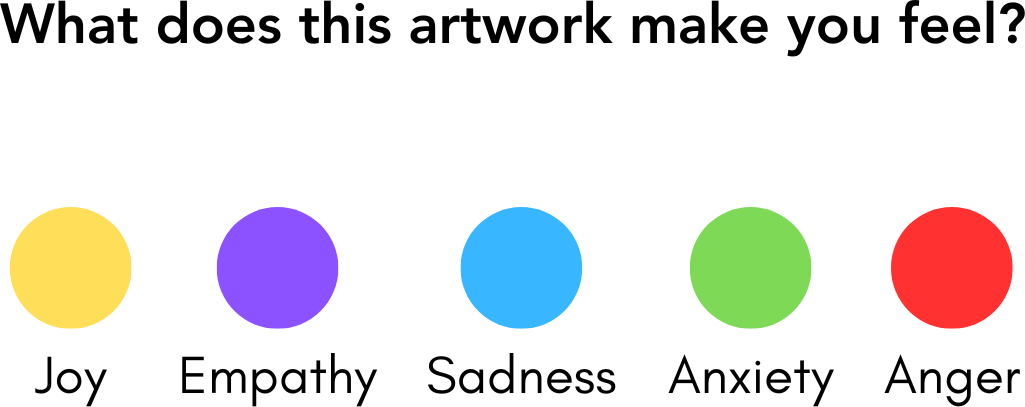
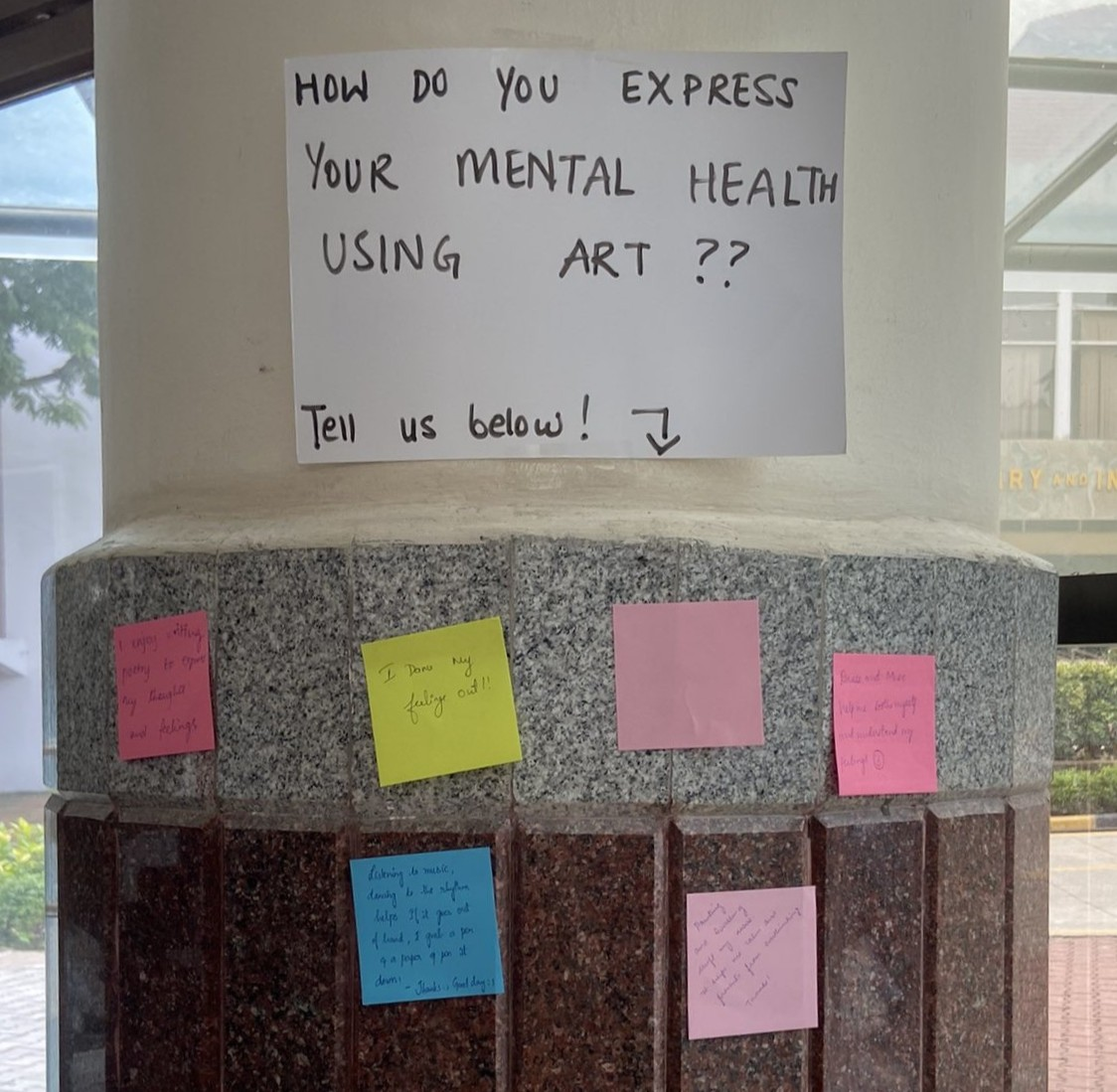
A second, larger exhibition was held during CBM-NIMHANS Brain Awareness Week celebrations, where we expanded the theme to include all mental illnesses and introduced dot-voting as an evaluation method (Figure 2a). Volunteers facilitated discussions with visitors around the artwork, focusing on the emotions they evoked, and encouraged visitors to share their reflections using sticky notes (Figure 2b).
3 Creative outputs and participant reflections
3.1 “Rewriting the narrative on mental illness” creative expression workshop
Thirty-seven people attended in person, with nine joining virtually (Table 2). Registrant (n=52) expectations focused on gaining knowledge (n=11), challenging myths, reducing stigma and/or raising awareness (n=8). Others cited additional motivations like collaboration opportunities, caregiver support and advocacy information. ‘Registrants’ refers to those who completed advance registration; ‘participants’ refers to those who attended the event (walk-ins + registrants).
|
Event |
Total Registra tions | Attendees | Participant Gender |
Age
Range (in years) |
|||
|
In-Person |
Virtual |
Female |
Male |
Prefer Not to Say | |||
|
Creative Expression Workshop |
52 |
37* |
9 |
Unavail- able |
Unavail- able |
Unavail- able |
19–61 |
|
World Bipolar Day Zine-Making Workshop |
48 |
42 |
N/A |
37 |
11 |
0 |
Unavail- able |
|
World Bipolar Day Art Exhibition |
50** |
∼70 |
N/A |
43 |
6 |
1 |
13–64 |
|
Brain Awareness Week Art Exhibition |
45** |
∼100 |
N/A |
38 |
5 |
2 |
18–45 |
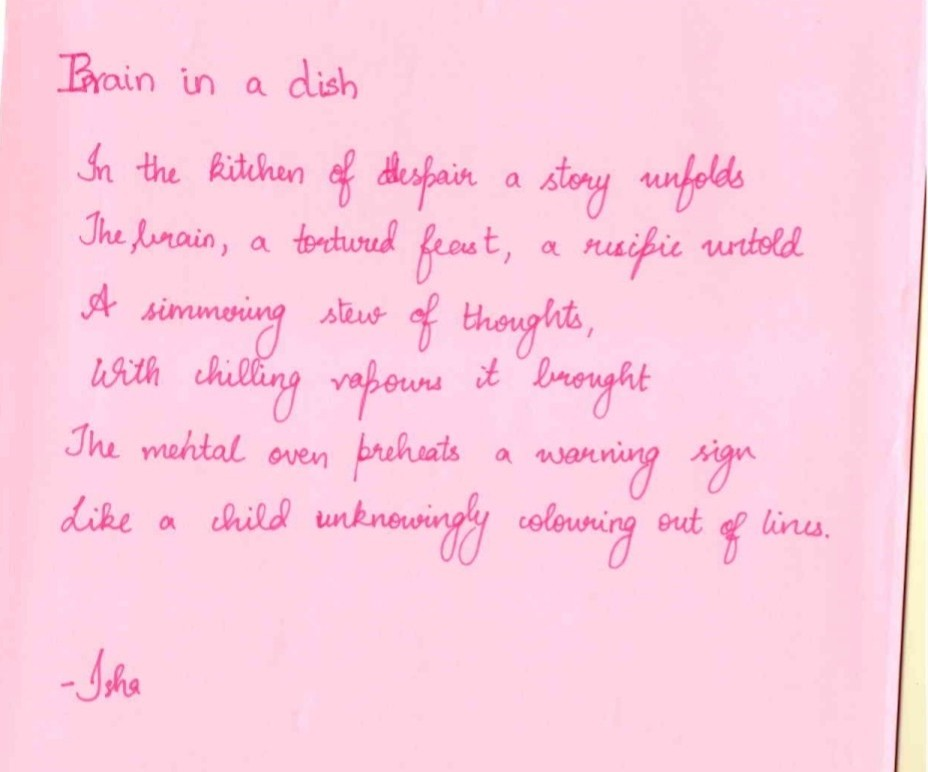
Participants produced 54 creative outputs (see Figure 3) across formats and languages. Subsequently, artworks were amplified through our social media channels and a blog post ( https://www.cbmnimhans.org/post/unveiling-perspectives-world-bipolar-day-recap) on our website.
3.1.1 Key discussion topics
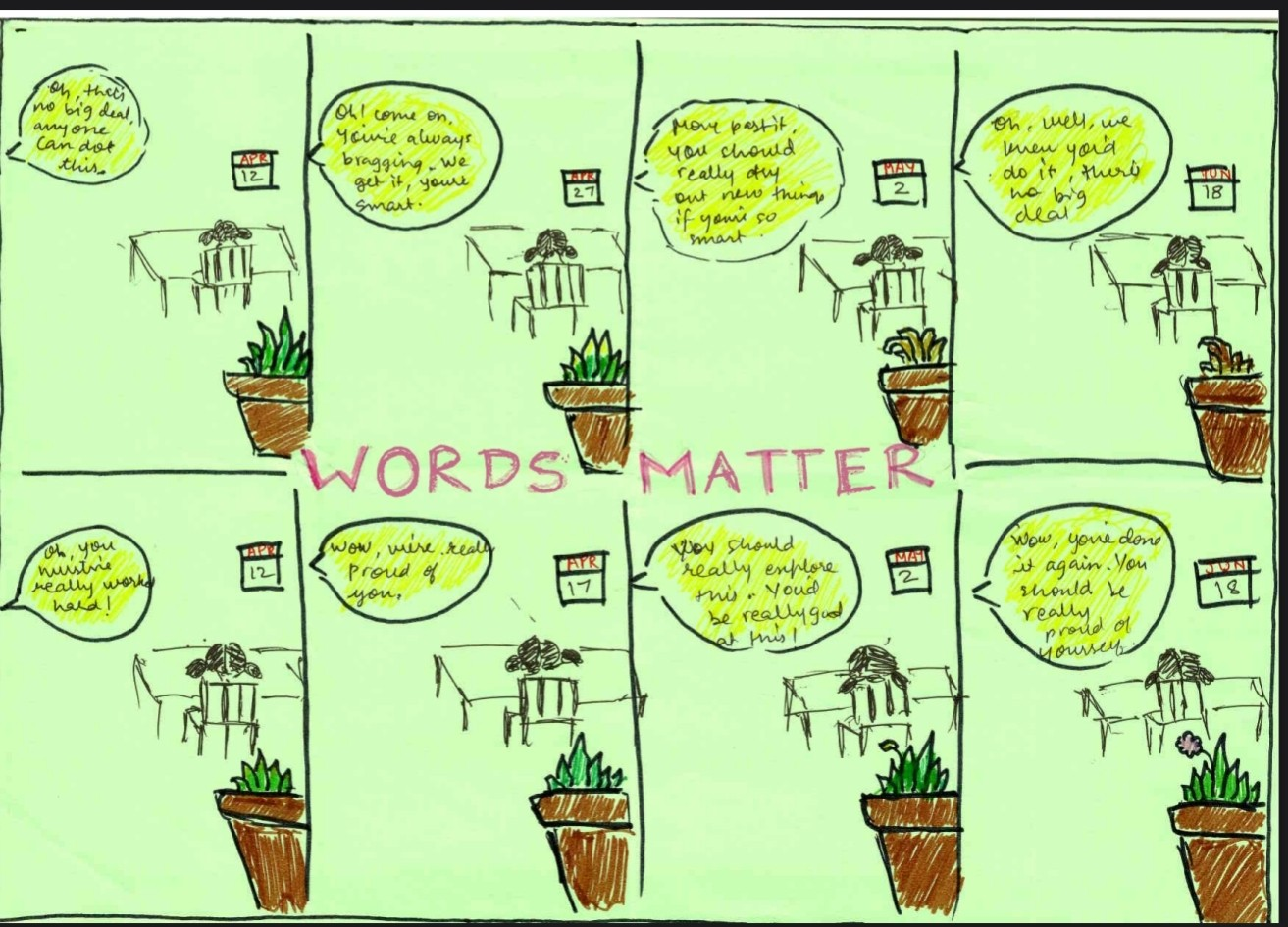
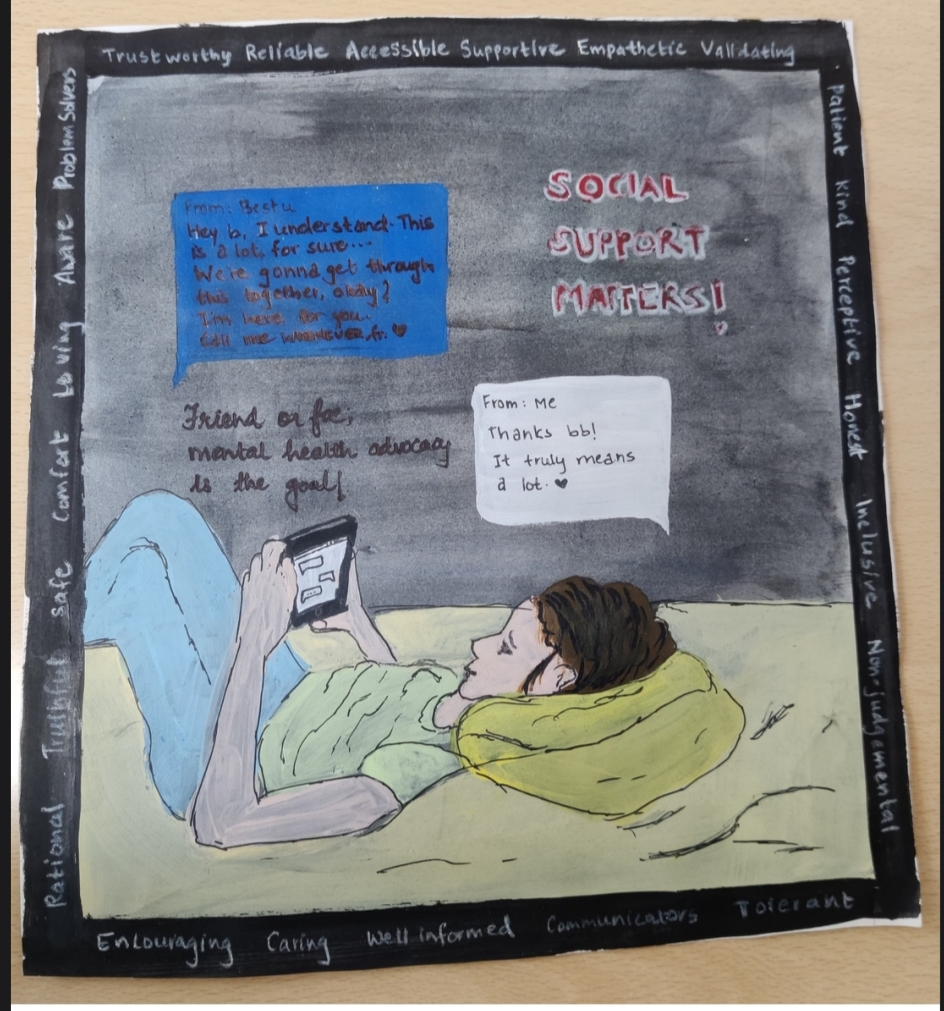
Discussions during the event centred on PwLEs’ real-world concerns. For instance, one participant, a mother, shared her difficulty in discussing her child’s developmental disorder with her family due to their denial, and how this lack of acceptance had prevented her child from receiving timely help. One of the speakers, a child and adolescent psychiatrist, offered guidance on navigating family conversations and the importance of sustained support for the child. In the same vein, other artworks created at the event reflected the importance of words for a child during formative years (Figure 3a).
Another participant expressed uncertainty about offering support as someone outside the immediate family, but who wished to play a meaningful role. In response, a psychiatrist emphasised the importance of holding space to listen, encouraging professional help and, where possible, accompanying the friend while seeking support.
PwLE also contributed insights to help address common challenges. For instance, one of the PwLE speakers shared her experiences of living with bipolar disorder, including the role of support systems and strategies she relies on to manage her condition.
3.1.2 Feedback
We collected participant feedback using both closed and open-ended questions. Participants found the information provided to be accessible and valued interactions between professionals and PwLE (e.g., the “interaction between professionals and PwLE on the same platform,” “narrating real experiences” and “sharing of new concepts by participants”). Suggestions for improvement included providing more time for small group discussions. This suggests that while hybrid and one-to-many formats can enable visibility, they may limit reciprocal dialogue.
3.2 Zine-making perception workshop: small group dialogue in practice
Forty-eight individuals registered for the event (Table 2), with participants displaying a mix of creative and knowledge-seeking expectations: exploring zine-making (n=24), getting insights into bipolar disorder and mental health (n=22) and gaining new knowledge (n=21). Conversations revealed some participants to be caregivers or PwLE of bipolar disorder.
Participants were asked how they might approach a person with bipolar disorder (see Table 1). One participant initially wrote, “learn their triggers.” However, after conversations with PwLE, they wrote, “approach calmly and shower them with love and support.” Another simply concluded, “Be a good friend, go hang out with them.”
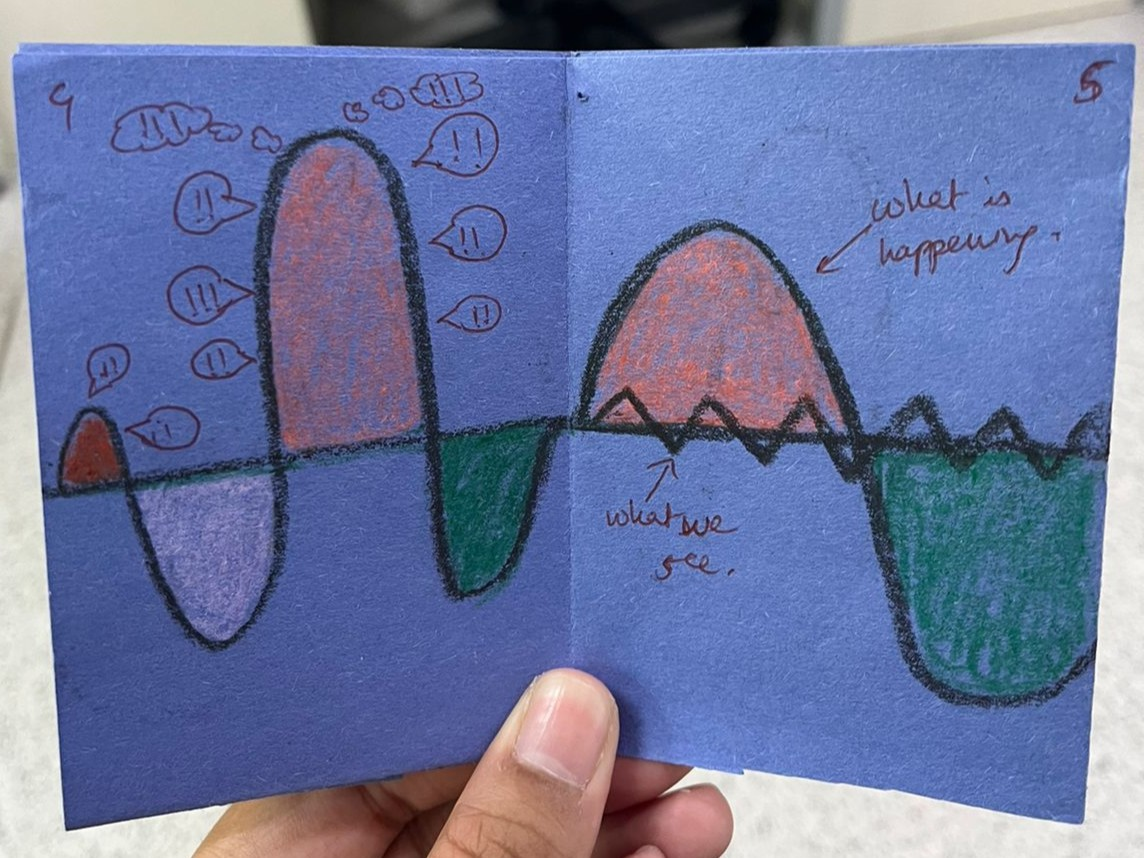
The zines captured participant perceptions before and after conversations with PwLE. Initially, participants tended to depict bipolar disorder through binaries of manic “highs” and depressive “lows.” By the end of the workshop, depictions reflected an understanding of bipolar disorder through the lens of PwLE (Figure 4).

3.2.1 Key discussion topics
Open discussions enabled PwLE to share lived experiences of stigma, diagnosis and daily life. At one table, school students asked about managing academic stress and how these challenges affected their condition. PwLE responded candidly about their struggles and the coping mechanisms they developed. Another shared that her family initially struggled to accept her diagnosis, partly due to societal stigma. However, open conversations helped them come to terms with it and better understand the difficulties she faced. A participant at the same table shared personal experiences closely echoing these reflections, creating a moment of shared understanding.
Participants asked about symptoms of bipolar disorder and how they vary among individuals and sought to understand other neurological and psychiatric aspects of the disorder. Participants also expressed interest in how PwLE balance treatment with daily life. Conversations also extended to hobbies and long-term career aspirations, reflecting participants’ interest in the lives of PwLE beyond diagnosis.
3.2.2 Feedback
Of the 13 participants who submitted feedback, most expressed high satisfaction. Participants reported that interactions with PwLE contributed to shifts in understanding. One participant reflected: “Before talking to her (a PwLE), I had a completely different opinion, and it changed when we had a conversation regarding the disorder.” Others emphasised that the workshop “debunked myths”, “helped me separate the person from the condition” and “made me more empathetic”.
PwLE speakers also reported positive experiences. One noted, “I was scared of receiving negative feedback. However, the small group format helped me open up and be vulnerable.” Another reflected: “talking about my experience in such a setting helped build strength and self-confidence.” These observations suggest the value of small-group, PwLE-led formats that centre shared experiences, which may help create common ground and support more nuanced understandings.
3.3 Art exhibitions
At the World Bipolar Day exhibition, 47 pieces of artwork were curated and displayed (Figure 5), reflecting a wide range of themes, including: Recovery (n=16), Struggle (n=8), Expression (n=7) and Identity (n=4), among Other topics (n=12). The event was attended by approximately 70 visitors (Table 2). Nine out of 15 visitors who gave feedback indicated high satisfaction (5 on a 5-point scale).
The Brain Awareness Week exhibition had 95 pieces of artwork on display (Figure 6), attracting more than 100 visitors (Table 2). A strong focus on Recovery (n=23 artworks), Struggle (n=20), Expression (n=34) and Identity (n=14) was evident, along with a few works tackling ‘Other’ themes (n=4).


With artists’ permission, postcards of selected artworks were made available for purchase, with proceeds going directly to them. One participant also displayed and sold an original painting. Visitors left supportive notes alongside their payments, and artists expressed appreciation for the platform and encouragement they received. This suggests that enabling recognition and ownership of creative work can deepen audience engagement (Supplementary Figure 2 in the supplementary material).
Visitor testimonials emphasised the variety and impact of the artworks, describing the works as “inspiring” and “thought-provoking.” As one participant noted:
I was blown aback when I saw the paintings different people had created regarding bipolar disorder. This topic is quite sensitive, vast and good, yet can be bad, which I saw in everyone’s painting that day. This showcased their creativity on a platform where everyone can see, which I like.
Artists remarked on the exhibition as a unique platform for visibility and self-expression.
I have never allowed myself to feel the value of things I am good at because I’ve been lied to, from my version of the world, about the concept of things that should be valuable and things that should not. The exhibition made me realise I am way too harsh on myself, and that’s half of the problem and that creative expression is the start of my healing journey.
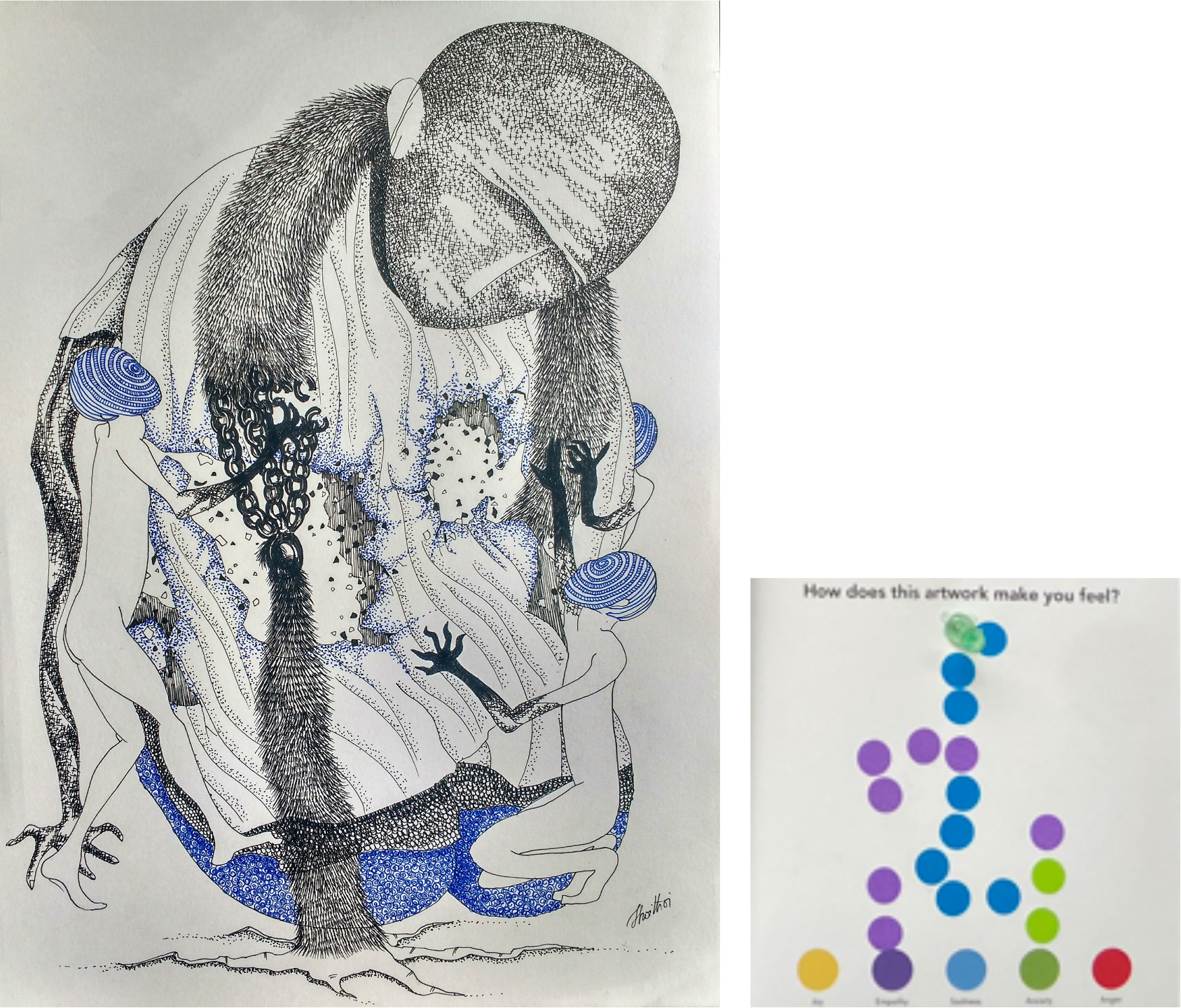
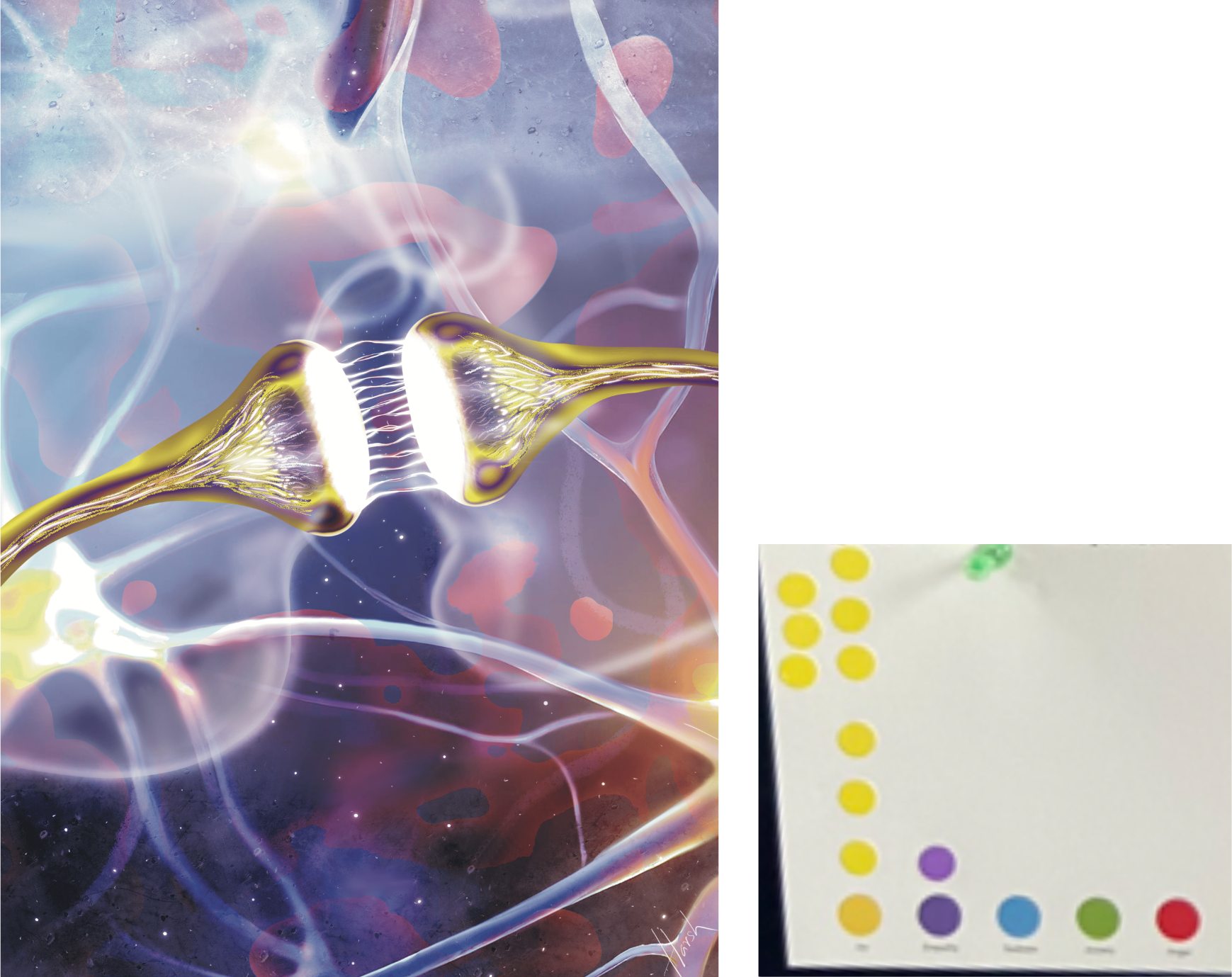
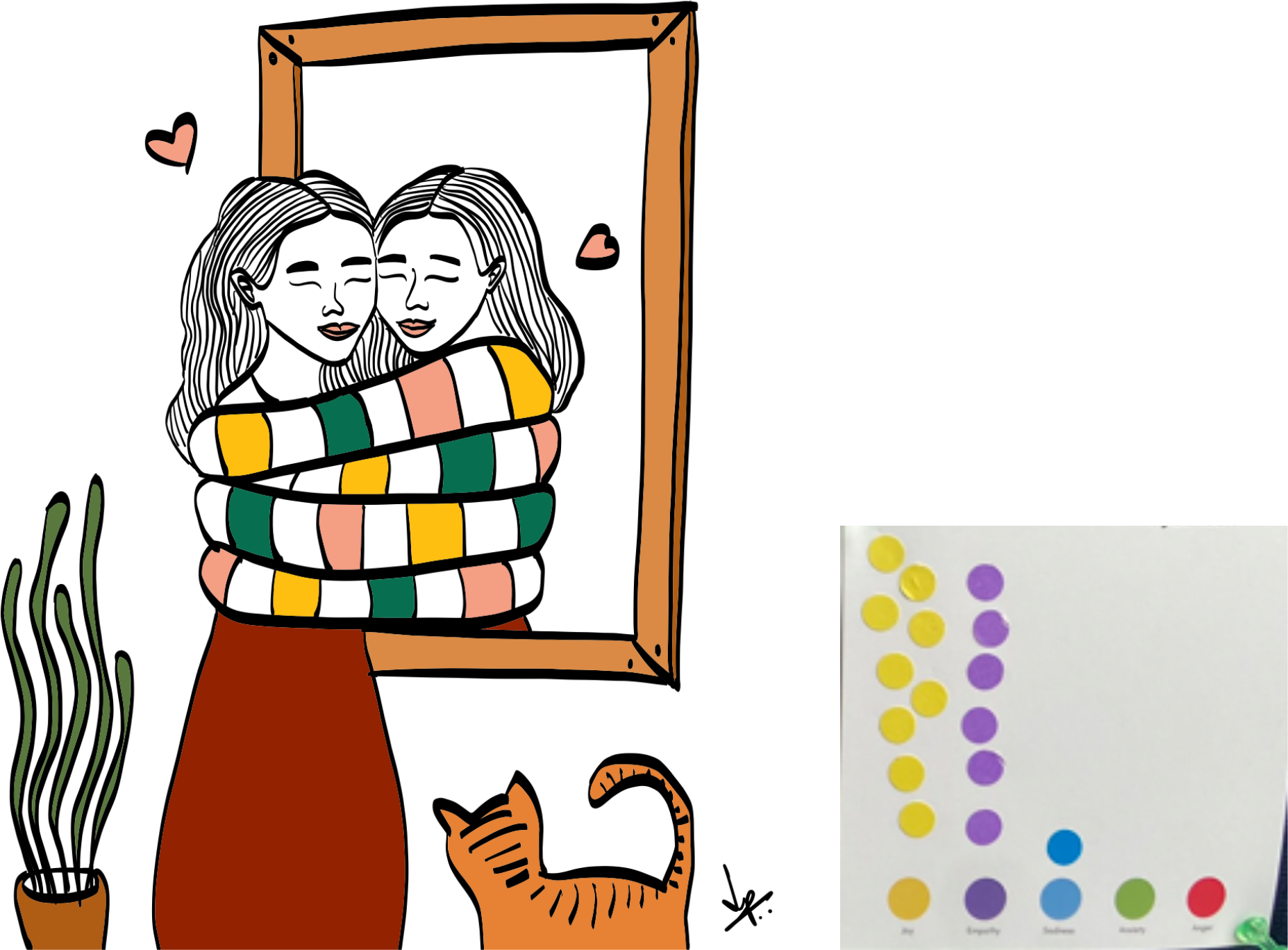
Visitors’ dot-voting aligned closely with artwork themes, suggesting empathetic engagement (Supplementary Table 1 in the supplementary material). For instance, Fleeting Moment (Figure 6a), which tackled the theme of Struggle, primarily evoked Sadness (Blue) and Empathy (Purple), with some Anxiety (Green). In contrast, artworks about Recovery, such as Art of Self Love (Figure 6b) and Embrace of Self (Figure 6c), predominantly elicited Joy (Yellow) and Empathy (Purple).
Visitor testimonials reflected on the exhibition’s dual role as a space for both awareness and artistic expression, with phrases like “a brilliant way to spread awareness” and reported being “glad to know that people express their emotions and thoughts through art.” Artists valued the exhibition as a platform for sharing experiences that had previously been missing.
4 Discussion
Our Practice Insight offers a novel way to address the challenges associated with mental illness communication by pairing participatory approaches with contact theory. This theory is a well-established framework in psychology and psychiatry [Corrigan & Shapiro, 2010; Stacciarini et al., 2011; Wallerstein & Duran, 2010], but has received little, if any, attention within science communication research and practice. We illustrate a transition towards dialogic and equal-status forms of communication that address cultural barriers and centre lived experience.
Our approach positioned PwLE as experts, while clinicians engaged as listeners and co-learners. This contrasts with the hierarchical doctor-patient dynamic prevalent in India, which prioritises expert knowledge while overlooking experiential contributions of PwLE. To support more equitable exchange of perspectives and knowledge, we structured the events in a small-group format. The positive feedback we received affirms the value of initiating dialogue through questions rooted in lived experience, rather than in expert assumptions.
Discussions captured in our events suggested that forums to ask questions, share uncertainty and reflect on mental health without fear of judgment are urgently needed. For many participants, especially young people, conversations about diagnosis, symptoms, or treatment are often difficult to initiate within families. Attendance by parents and caregivers suggested that such workshops can act as platforms for these conversations as well.
Our events spanned a variety of art-based engagement modalities. We aimed to diversify participant involvement and foster engagement with the human, emotional aspect of mental illness. The creative expression workshop demonstrated the value of culturally relevant communication approaches — for instance, the use of a skit, a popular approach to discuss social issues in public spaces in India. In the zine-making workshop, the “before-and-after” component let participants reflect on their views, from preconceived ideas (“before”) to a more humanistic stance (“after”). With the art exhibitions, PwLE could express their perspectives while controlling disclosure, thereby reducing risks associated with their public participation.
In India, where public discussions of mental illness are severely constrained, art may offer a socially acceptable and emotionally accessible entry point. Creative works (zines, comics, poems, skits, exhibitions) reflected how participants understood lived experience, particularly PwLEs’ individuality beyond diagnosis and the presence of support systems. Amorphous thoughts became tangible outputs and could be further analysed. By analysing dot-voting results and written notes from visitors, we observed that visitors were able to empathise with the artist. This was further reflected in visitors’ willingness to purchase original artwork and postcards. Strong interest from the participating public in attending similar events in the future suggests potential for sustained public engagement.
Several constraints shaped this work. The initial participant evaluation we collected was primarily qualitative and, while useful, was also uneven. Further, response rates were often low, limiting comparability across events and making it difficult for us to assess the extent or sustainability of observed changes. These considerations highlight the need for more consistent, accessible and mixed-method evaluation approaches. As the work evolved, we iteratively refined our evaluation approaches to be more consistent, less cumbersome and embedded from the outset.
Participants were also mostly younger, urban and digitally connected, which constrains transferability to other contexts. This necessitates more inclusive formats and steady involvement of PwLE beyond one-time events. In our future efforts, we are adapting diverse formats across multiple languages and literacy levels, alongside our ongoing work to develop sustained engagement with the PwLE by building a PPIE community for mental illnesses in India (Appendix 2 in the supplementary material).
4.1 Learnings for science communication practice
Through these events, we found that bringing clinicians and PwLE together can reduce hesitation around asking sensitive questions, consistent with evidence that contact aids the reduction of stigma-related anxieties [Pettigrew & Tropp, 2006]. Small, in-person group settings anchored by PwLE could enable deeper dialogue and engagement. Creative formats also shape how audiences engage with stigmatised topics.
Art exhibitions can lower the threshold for engagement, particularly for those hesitant to speak directly [Mendon et al., 2024]. Emerging evidence from PwLE-developed CREATORS program in India similarly corroborated the feasibility and impact of such approaches in reducing stigma [Gaiha et al., 2024]. We suggest that these formats can serve as inclusive and reflective science communication strategies to engage with other health-related topics steeped in societal stigma [CPAS Inclusive Science Communication Collective, 2025; Gronholm et al., 2024].
4.2 Conclusion
This Practice Insight offers perspectives on how prioritising lived experiences, promoting shared authority and using art as a medium can lower hesitation towards dialogue and participation — especially in stigmatised contexts. These approaches may facilitate knowledge sharing and engagement among diverse stakeholders, who often lack opportunities to exchange ideas. Approaches relying on small-group, facilitated dialogue and arts-based participation can be reproduced; however, ensuring adaptation and sensitivity across contexts is imperative.
Although well documented in mental health and sociological research, the role of shame and dishonour as a barrier to meaningful participation remains underexplored in science communication literature. In such contexts, the challenge often lies not in a lack of information but in creating conditions where engagement feels safe and meaningful. Science communicators must treat stigma not only as an outcome to be addressed, but as a factor that shapes participation itself. By recognising this important barrier — and using approaches that help the public overcome it — we can ensure that efforts to communicate are participatory, equitable and sustainable.
Acknowledgments
We thank all participants, especially PwLE, for sharing their experiences, and the artists for allowing us to use their artwork. We thank Shatabdi Pal, Chitra Kadu and Mesha P S for administrative support. We thank the staff, students and office attenders of CBM-NIMHANS and the Molecular Genetics Lab for their support during our events. We acknowledge our 4th IndiaBioscience Outreach Grant (IOG) collaborators from Sangath India (Bhopal Hub), Mental Health Support Foundation, FAST India and Project Encephalon, and our International Brain Research Organisation (IBRO)/Dana Foundation Brain Awareness Week 2024 grant collaborators from the Department of Mental Health Education, NIMHANS and CBM-National Centre for Biological Sciences (NCBS). We acknowledge the institutional support of the NIMHANS, Bengaluru. This work was funded by the CBM-NIMHANS via Rohini Nilekani Philanthropies (G-202303-00523), SKAN Research Trust (SKAN/002/208/2021/01481), DBT/Wellcome Intermediate Fellowship (IA/CPHI/20/1/505266 to B.V), MQ: Transforming Mental Health Fellowship [(MQF22/20 to S.G.) and (2023-MPSIP-54 to A.S.N.M)], DST INSPIRE fellowship (DST/INSPIRE/04/2021/003250 to A.S.N.M), 4th IndiaBioscience Outreach Grant (IBS/2023/01719 to R.S.) and IBRO/Dana Brain Awareness Week Grant (BAW) 2024 (IBRO/2024/01788 to R.S.). Our workshops were supported by the India Science Festival, IOG, SKAN, BAW and CBM-NIMHANS. Salary support for A.B., B.M.S., I.Z., K.P., P.J., R.S., S.N. and V.T. was provided by CBM-NIMHANS. The funders had no role in the analysis or the preparation of the manuscript.
References
-
Allport, G. W. (1954). The nature of prejudice. Addison-Wesley.
-
Bucchi, M. (2008). Of deficits, deviations and dialogues: Theories of public communication of science. In Handbook of public communication of science and technology (pp. 71–90). Routledge. https://doi.org/10.4324/9780203928240-11
-
Bucchi, M., & Trench, B. (2021). Rethinking science communication as the social conversation around science. JCOM, 20(03), Y01. https://doi.org/10.22323/2.20030401
-
Corrigan, P. W., & Watson, A. C. (2002). Understanding the impact of stigma on people with mental illness. World Psychiatry, 1(1), 16–20.
-
Corrigan, P. W. (2020). Effect of contact-based interventions on stigma and discrimination. Psychiatric Services, 71(12), 1324–1325. https://doi.org/10.1176/appi.ps.711203
-
Corrigan, P. W., Mittal, D., Reaves, C. M., Haynes, T. F., Han, X., Morris, S., & Sullivan, G. (2014). Mental health stigma and primary health care decisions. Psychiatry Research, 218(1-2), 35–38. https://doi.org/10.1016/j.psychres.2014.04.028
-
Corrigan, P. W., & Shapiro, J. R. (2010). Measuring the impact of programs that challenge the public stigma of mental illness. Clinical Psychology Review, 30(8), 907–922. https://doi.org/10.1016/j.cpr.2010.06.004
-
CPAS Inclusive Science Communication Collective. (2025). A proposed framework for considering “inclusive science communication” in theory and practice. Science Communication, 10755470251344471. https://doi.org/10.1177/10755470251344471
-
Damsté, C., Gronholm, P. C., Groot, T. D., Gurung, D., Makhmud, A., Peters, R. M. H., & Hartog, K. (2024). Social contact as a strategy to reduce stigma in low- and middle-income countries: a systematic review and expert perspectives. PLOS Global Public Health, 4(3), e0003053. https://doi.org/10.1371/journal.pgph.0003053
-
Edward, M. (2025). Breaking the silence: addressing stigma in mental health. Discover Public Health, 22(1), 441. https://doi.org/10.1186/s12982-025-00803-3
-
Einsiedel, E. F. (2021). Public participation in science and technology: dialogue, disputations and collaborations. In M. Bucchi & B. Trench (Eds.), Routledge handbook of public communication of science and technology (3rd ed., pp. 267–290). Routledge. https://doi.org/10.4324/9781003039242
-
Gaiha, S. M., Gasparrini, A., Koschorke, M., Raman, U., Petticrew, M., & Salisbury, T. T. (2024). Impact, feasibility and acceptability of CREATORS: an arts-based pilot intervention to reduce mental-health-related stigma among youth in Hyderabad, India. SSM — Mental Health, 6, 100339. https://doi.org/10.1016/j.ssmmh.2024.100339
-
Gronholm, P. C., Kline, S., Lamba, M., Lempp, H., Mahkmud, A., Morales Cano, G., Vashisht, K., Vera San Juan, N., & Sunkel, C. (2024). Exploring perspectives of stigma and discrimination among people with lived experience of mental health conditions: a co-produced qualitative study. eClinicalMedicine, 70, 102509. https://doi.org/10.1016/j.eclinm.2024.102509
-
Gundi, M., Kaikobad, R., & Sharma, S. (2025). Diversity in approaches in community-based mental health interventions in India: a narrative review and synthesis. Cambridge Prisms: Global Mental Health, 12, e89. https://doi.org/10.1017/gmh.2025.10046
-
Gururaj, G., Varghese, M., Benegal, V., Rao, G. N., Pathak, K., Singh, L. K., Mehta, R. Y., Ram, D., Shibukumar, T. M., Kokane, A., Lenin Singh, R. K., Chavan, B. S., Dalal, P. K., Sharma, P., Saha, P. K., Deuri, S. P., Giri, A. K., Kavishvar, A. B., & Group, N. C. (2016). National mental health survey of India, 2015–16: prevalence, patterns and outcomes [NIMHANS publication no. 129]. National Institute of Mental Health; Neuro Sciences. https://indianmhs.nimhans.ac.in/phase1/Docs/Report2.pdf
-
Kågström, A., Guerrero, Z., Aliev, A. A., Tomášková, H., Rüsch, N., Ouali, U., Thornicroft, G., Sartorius, N., & Winkler, P. (2025). Mental health stigma and its consequences: a systematic scoping review of pathways to discrimination and adverse outcomes. eClinicalMedicine, 89, 103588. https://doi.org/10.1016/j.eclinm.2025.103588
-
Kaur, A., Kallakuri, S., Kohrt, B. A., Heim, E., Gronholm, P. C., Thornicroft, G., & Maulik, P. K. (2021). Systematic review of interventions to reduce mental health stigma in India. Asian Journal of Psychiatry, 55, 102466. https://doi.org/10.1016/j.ajp.2020.102466
-
Kirpekar, V., Faye, A., Bhave, S., Gawande, S., & Tadke, R. (2024). District mental health program: then and now. Indian Journal of Psychiatry, 66(7), 603–613. https://doi.org/10.4103/indianjpsychiatry.indianjpsychiatry_974_23
-
Majeed, T., Hopkin, G., Wang, K., Nepal, S., Votruba, N., Gronholm, P., Gurung, D., Semrau, M., Bagade, T., Farina, N., Musyimi, C., Pingani, L., Breuer, E., Lund, C., Thornicroft, G., & Evans-Lacko, S. (2024). Anti-stigma interventions in low-income and middle-income countries: a systematic review. eClinicalMedicine, 72, 102612. https://doi.org/10.1016/j.eclinm.2024.102612
-
Mendon, G. B., Gurung, D., Loganathan, S., Abayneh, S., Zhang, W., Kohrt, B. A., Hanlon, C., Lempp, H., Thornicroft, G., & Gronholm, P. C. (2024). Establishing partnerships with people with lived experience of mental illness for stigma reduction in low- and middle-income settings. Cambridge Prisms: Global Mental Health, 11, e70. https://doi.org/10.1017/gmh.2024.69
-
Metcalfe, J., Gascoigne, T., Medvecky, F., & Nepote, A. C. (2022). Participatory science communication for transformation. JCOM, 21(02), E. https://doi.org/10.22323/2.21020501
-
Pettigrew, T. F., & Tropp, L. R. (2006). A meta-analytic test of intergroup contact theory. Journal of Personality and Social Psychology, 90(5), 751–783. https://doi.org/10.1037/0022-3514.90.5.751
-
Raghavan, V., Chandrasekaran, S., Paul, V., Pattabiraman, R., Mohan, G., Durairaj, J., Currie, G., Lilford, R., Furtado, V., Madan, J., Birchwood, M., Meyer, C., Sood, M., Chadda, R., Mohan, M., Shah, J., John, S., Padmavati, R., Iyer, S., … Singh, S. (2024). Effectiveness of a mental health literacy module on stigma related mental health knowledge and behaviour among youth in two educational settings in Chennai, South India: a quasi-experimental study. Asian Journal of Psychiatry, 98, 104074. https://doi.org/10.1016/j.ajp.2024.104074
-
Rai, S., Gurung, D., & Kohrt, B. (2023). The PhotoVoice method for collaborating with people with lived experience of mental health conditions to strengthen mental health services. Cambridge Prisms: Global Mental Health, 10, e80. https://doi.org/10.1017/gmh.2023.73
-
Samudre, S., Shidhaye, R., Ahuja, S., Nanda, S., Khan, A., Evans-Lacko, S., & Hanlon, C. (2016). Service user involvement for mental health system strengthening in India: a qualitative study. BMC Psychiatry, 16(1), 269. https://doi.org/10.1186/s12888-016-0981-8
-
Sartor, C. (2023). Mental health and lived experience: the value of lived experience expertise in global mental health. Cambridge Prisms: Global Mental Health, 10, e38. https://doi.org/10.1017/gmh.2023.24
-
Seethaler, S., Evans, J. H., Gere, C., & Rajagopalan, R. M. (2019). Science, values and science communication: competencies for pushing beyond the deficit model. Science Communication, 41(3), 378–388. https://doi.org/10.1177/1075547019847484
-
Shidhaye, R., & Kermode, M. (2013). Stigma and discrimination as a barrier to mental health service utilization in India. International Health, 5(1), 6–8. https://doi.org/10.1093/inthealth/ihs011
-
Simis, M. J., Madden, H., Cacciatore, M. A., & Yeo, S. K. (2016). The lure of rationality: why does the deficit model persist in science communication? Public Understanding of Science, 25(4), 400–414. https://doi.org/10.1177/0963662516629749
-
Stacciarini, J.-M. R., Shattell, M. M., Coady, M., & Wiens, B. (2011). Review: community-based participatory research approach to address mental health in minority populations. Community Mental Health Journal, 47(5), 489–497. https://doi.org/10.1007/s10597-010-9319-z
-
Thornicroft, G., Mehta, N., Clement, S., Evans-Lacko, S., Doherty, M., Rose, D., Koschorke, M., Shidhaye, R., O’Reilly, C., & Henderson, C. (2016). Evidence for effective interventions to reduce mental-health-related stigma and discrimination. The Lancet, 387(10023), 1123–1132. https://doi.org/10.1016/s0140-6736(15)00298-6
-
Thornicroft, G., Sunkel, C., Alikhon Aliev, A., Baker, S., Brohan, E., el Chammay, R., Davies, K., Demissie, M., Duncan, J., Fekadu, W., Gronholm, P. C., Guerrero, Z., Gurung, D., Habtamu, K., Hanlon, C., Heim, E., Henderson, C., Hijazi, Z., Hoffman, C., … Winkler, P. (2022). The Lancet commission on ending stigma and discrimination in mental health. The Lancet, 400(10361), 1438–1480. https://doi.org/10.1016/s0140-6736(22)01470-2
-
Wallerstein, N., & Duran, B. (2010). Community-based participatory research contributions to intervention research: the intersection of science and practice to improve health equity. American Journal of Public Health, 100(S1), S40–S46. https://doi.org/10.2105/ajph.2009.184036
Notes
1. These authors contributed equally to this work.
About the authors
Kadambari Patil is a science communicator and illustrator with a background in Zoology and Botany. As the visual communication lead at the Centre for Brain and Mind - NIMHANS, she ensures complex scientific information is accessible and engaging across platforms. She has secured grants for outreach, curated science-art exhibitions, and coordinated neuroscience public engagement programs. Her work extends to Public Patient Involvement and Engagement (PPIE), centering lived experience in research and communication.
E-mail: writetokadambari7900@gmail.com Bluesky: @kadambarii
Anushka Banerjee is a molecular biologist-turned science communication and public engagement practitioner with over five years of experience at the intersection of neuroscience, mental health and society. She leads communication and outreach initiatives at the Centre for Brain and Mind-NIMHANS. Her work focuses on translating complex research for diverse audiences across audio-visual formats and creating programmes for meaningful collaboration between researchers, people with lived experience, and wider communities to make science more accessible and relevant. She has co-led the securing and execution of outreach grants on non-animal research methods and mental health awareness.
E-mail: banerjeee.anushka@gmail.com Bluesky: @anushkabanerjee
Imtiaz Zafar. Neuroscientist, stem cell researcher and mental health activists working on IPSC based disease modeling of neuropsychiatric disorders.
E-mail: imtiaz.stem@gmail.com
Ipsa Jain. Scientist turned freelance science communicator. Interested in perception of science, process of science and molecular science.
E-mail: ipsajain.31@gmail.com
Meghna Prakash — Meghna Prakash (she/they) is a counselling psychologist, lived-experience researcher, and co-founder of Soft Spaces Therapy, India. Her work sits at the intersection of critical psychology, epistemic justice, and clinical practice. She brings a decolonial and neurodivergent-affirming lens to questions of trauma, identity, and mental health.
E-mail: meg@softspacestherapy.in
Pavithra Jayasankar — Dr. Pavithra Jayasankar is an Assistant Professor at the Centre for Brain and Mind, Department of Psychiatry, NIMHANS, India. She holds an MD in Psychiatry and a Post-Doctoral Fellowship in Neuropsychiatry, with over six years of post-MD experience. Her research spans epidemiology of psychiatric illness, cognition, severe mental illnesses including schizophrenia and bipolar disorder, and the use of near-infrared spectroscopy in psychiatry. A gold medallist and award-winning researcher with 20+ publications (H-index: 6), she is also actively involved in patient and caregiver outreach.
E-mail: mayurvanish@gmail.com
Varsha Kini. A staunch advocate of Mental Health literacy and a person with lived experience. Guides people on how to manage mental health in high stress environment.
E-mail: kinivarsha@gmail.com
Vasundhra Teotia — Dr. Vasundhra Teotia completed her postgraduate training in Psychiatry at NIMHANS and later pursued a fellowship in Obsessive-Compulsive and Related Disorders. Her clinical interests focus on OCD and related disorders. She has worked with Centre for Brain and Mind, NIMHANS with a research interest in endophenotypic markers within multiplex family cohorts. She is currently working as a Psychiatry Registrar at Western Health, Melbourne. She combines clinical practice with research and is committed to evidence-based, patient-centred care and continuous professional development.
E-mail: vasundhrat@gmail.com
Ashitha Siddappa Niranjana Murthy — Dr. Ashitha S.N.M. is a neuroscience researcher whose work focuses on the genetic and molecular basis of neurodevelopmental and psychiatric disorders, particularly autism spectrum disorder, schizophrenia and bipolar disorders. Alongside her research, she is actively involved in science communication and public outreach engagements. She has contributed to outreach initiatives including Manotsava and Pint of Science, where she works to make complex topics in neuroscience, genetics, and mental health accessible to diverse audiences. Her interests lie in bridging research, clinical practice, and public understanding of brain health.
E-mail: ashithasnm09@gmail.com
Bhagyalakshmi Mallapura Shankarappa — Dr. Bhagyalakshmi Shankarappa is a Project Scientist at the Molecular Genetics Lab, Center for Brain and Mind, NIMHANS, Bangalore. Her research focuses on the genetics and epigenetics of neuropsychiatric disorders. She completed her Ph.D. on genetic and epigenetic correlates of alcohol-induced liver cirrhosis and she has authored peer-reviewed publications in journals including DNA and Cell Biology and the Journal of Human Genetics. And she is actively involved in patient and public involvement (PPI) initiatives in mental health research. A recipient of multiple international awards including the Young Investigator award from SOBP, WFSBP, EMBO Travel Grant and ACNP Global Scholarship, she is an active member of ISPG, RSA, and PGRN.
E-mail: bhagyalakshmishankarappa@gmail.com
Swarna Buddha Nayok — I am an Assistant Professor in the Department of Clinical Psychopharmacology and Neurotoxicology at NIMHANS, Bengaluru. I hold an MD in Psychiatry, and a Ph.D. in Clinical Neurosciences. My research interests span neuroimaging, neurophysiology, neuromodulation, psychopathology, psychopharmacology, and clinical neuroscience. I am particularly interested in leveraging multimodal data and advanced analytical approaches to better understand psychiatric disorders. Beyond clinical and translational neuroscience, I am also interested in science communication, media psychology, and cultural psychiatry, with a focus on bridging research, public engagement, and mental health awareness.
E-mail: swarnabuddha_nayok@yahoo.co.in
Jayant Mahadevan — Dr. Jayant Mahadevan is Assistant Professor of Psychiatry at the Centre for Addiction Medicine at NIMHANS, Bangalore. He did his MBBS and MD in Psychiatry from JIPMER, Pondicherry and DM in Addiction Psychiatry from NIMHANS. He is a passionate clinician and enjoys working with young people with substance use and individuals with co-occurring psychiatric illness and substance use. He is also involved in teaching, training and capacity building in the area of substance use disorders for both specialists and non-specialists. His research centers primarily around understanding biological and environmental vulnerability to psychiatric illness, substance use disorders and substance use related medical problems. He has also been actively involved in science communication and delivers talks to the general public on psychiatric illness and substance use.
E-mail: jayantmahadevan@gmail.com
Suhas Ganesh — Dr Suhas Ganesh is a clinician-scientist and MQ: Transforming Mental Health Fellow at the National Institute of Mental Health and Neurosciences. He is the recipient of NARSAD Young Investigator Award from the Brain and Behaviour Research Foundation and MQ fellowship from MQ UK. His research focuses on genomics in severe mental illnesses.
E-mail: suhasg90@gmail.com
Biju Viswanath — I am a Professor of Psychiatry at NIMHANS, Bengaluru, with training in both clinical psychiatry and human stem cell research. This dual expertise drives my focus on the molecular basis of etiology and treatment response in neuropsychiatric disorders. My current work examines genetic and cellular correlates of lithium response in bipolar disorder. I serve as a key investigator at the Rohini Nilekani Centre for Brain and Mind at NIMHANS, lead a network of psychiatric genetics investigators across India, and am a DBT/WT India Alliance Intermediate Fellow.
E-mail: cbm.nimhans@gmail.com
Reeteka Sud — a Senior Scientist (Research Associate Professor) at the Centre for Brain and Mind, Dept. of Psychiatry at NIMHANS, Dr. Sud’s expertise lies at the intersection of Genetics, Neuroscience and Psychiatry. Her passion for bringing knowledge from scientific publications into popular domain forms the basis of her participation in scicomm initiatives. For the same reason, she also co-leads the burgeoning Patient-Public Involvement program at CBM-NIMHANS.
E-mail: reeteka@gmail.com Bluesky: @reeteka
Supplementary material
Available at https://doi.org/10.22323/352620260511100542
Supplementary appendices 1 and 2, figures 1 and 2 and table 1